Considering
Facelift Surgery?
So you’ve been considering facelift surgery for a while now, maybe put the idea to bed a few times, even tried non-surgical options but keep coming back to it.
You’ve scoured the internet for information, been on cosmetic surgery review sites, seen dozens of stock photographs of models with youthful faces and still feel none the wiser.
Well relax you have now found the definitive facelift guide that will hopefully clear the fog and cut through all the marketing and hype to explain facelifting.


What is a
Facelift?
Simply put, a face lift is a cosmetic surgical procedure that lifts the deeper tissues of the face and neck back to a more youthful position, creating excess skin which is removed and the skin is stitched back together.
Sounds simple right? As always the devil is in the detail. All surgeons make incisions and all put the closing stitches in. The difference lies in the words
lifts the deeper tissues of the face and neck
Types of Facelift
Let’s assume that all surgeons make incisions, the positioning of these varies depending on surgeon and procedure, but generally the surgeon will make ones that perfectly follow the contours in front of the ear, turn around the earlobe, then pass up the back of the ear into the hairline.
The excess skin is then elevated off the SMAS (Superficial musculoaponeurotic system) which is a fascial layer that envelopes the facial muscles and continues as the platysma muscle in the neck – the one that causes vertical neck bands.
The fact the SMAS and Platysma are continuous lends weight to my argument that one shouldn’t have a face lift without a neck lift and viceversa. The face and neck were born together, have aged together and should be rejuvenated together for a natural rejuvenation.
Once the skin is elevated, this is when the facelift surgery actually starts. The skin is a passenger throughout and should play no role in support of a lifted face – it just goes along for the ride.
All surgeons do things slightly differently at this stage but all face lift techniques follow a theme. The options – in increasing complexity – for lifting the SMAS are as follows.

Mini facelift
There is no consensus in cosmetic surgery what a mini facelift actually means.
In general a mini facelift is a smaller version of an imbrication or a plication facelift. A minimal downtime, minimal recovery lift with reduced longevity and effect. Most trademarked facelifts fall within this mini facelift surgery category.
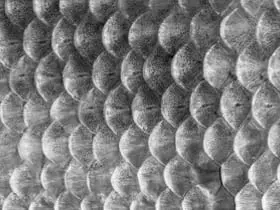
Imbrication
The SMAS is bunched together with a loop of purse-string suture and fixed in a higher position to immobile fascia in front of the ear and along the cheek bone. Think of fish scales which tightly overlap.
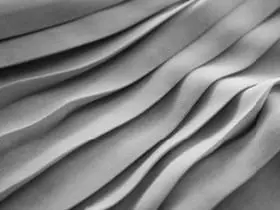
Plication
The SMAS is folded over and stitched to itself, either vertically, horizontally or obliquely, just like pleated fabric.

SMASectomy
A strip of SMAS is removed and the edges stitched together either vertically, horizontally or obliquely. Think of a gorge closing in on itself.

High SMAS or High lateral SMAS
An extended version of the SMASectomy that extends above the cheek bone and includes ligament dissection but the fulcrum of lift is distant to the jowl.

Deep plane facelift
Dissection under the SMAS starts further from the ears towards the centre of the face, the deep retaining ligaments of the face are released and now unhindered the neck, jowl and mid face move upwards together in a much more intuitive and natural vector.
The right
facelift?
Any of the above facelifts will work to a lesser or greater extent, and face lift results are dependent on the degree of ageing being treated and also the cosmetic surgeon’s artistry and technical competence.
Having performed all of the above face lift variants, my own surgical technical evolution has led me to the unequivocal conclusion.
deep plane facelift should be renamed correct plane facelift.

deep plane facelift should be renamed correct plane facelift.
SMAS lifts can lead to acceptable results, they produce a predictably tighter jawline and some neck improvement but do little for the descended midface, and often need additional plumping with autologous fat transfer and/or midface lifting.
They cannot comprehensively correct the anatomical cause of jowling and are prone to creating deformity of tension and vector leaving tell-tale signs of facelift surgery. The reason for this was they are pulling against several deep ligamentous anchors and do not directly approach the contour irregularities in the central face which patients had seek to correct.
Let me expand, and I am going to use my patient Helen to help me explain. When a patient points to their ageing face signs, their concerns (except lateral brow descent) are always located in the central three fifths of the face.

From top down, forehead wrinkles, upper eyelid hooding, rounded lower eye lids and scleral show, under eye bags, flattened mid face, descended malar fat pads, nasolabial folds, downturned mouth corners, marionette lines and jowls. In the neck, loose skin, platysma bands, deep neck fat, descended submandibular glands and loss of neck chin angle are located in the central three facial fifths as I have drawn on Helen.
Yet, plastic surgeons for decades have attempted to improve these centrally located concerns by tightening the lateral facial fifths by the ears. Compounding this paradox, between the target central three fifths and the actual operated lateral fifth lie the deep retaining ligaments of the face which prevent mobility of the target area when tightened laterally. You can feel this on your own face, the jowl and central cheek is mobile, the skin in front of the ear less so.
A composite (skin and SMAS) deep plane lift carefully releases these facial anchors allowing an access to the central portion of the face where the ageing concerns are present, with the retaining ligaments divided, the face and neck are free to be lifted to a position of youth unhindered by dense anchors. This release, coupled with deep central neck reduction if necessary yields a natural and beautiful rejuvenation.
if your cosmetic surgeon isn’t doing deep plane ask why?
You might not be getting the best cosmetic surgery approach
I can hear you thinking. If it’s that unequivocal why isn’t every face lift deep plane only. The answer is twofold. Firstly, young patients, or those with milder facial ageing can do very well with more superficial lifts but secondly, and most importantly, only a small percentage of surgeons performing facelifts worldwide will enter the deep plane. It is technically more complex, there is a learning curve and a surgeon needs experience and complete comfort in the face which only comes with sub-specialisation.
Non deep plane facelift surgeons will counter that the risks are higher, the cosmetic surgery is amongst facial nerve branches and the recovery is longer. I know this mantra as I used to be among their voice and still hear it at conferences! In reality, the few facelift surgeons regularly doing composite deep plane facelifts are more experienced, have technically evolved and have a lower rate of nerve injury, haematoma, seroma and skin necrosis then the wider cohort of more superficial SMAS level face lift surgeons.
What makes a great facelift?
There are lots of good facelifts around, which is why the bad ones make the media. A good facelift will leave the patient looking a younger fresher version of themself.
A great facelift will leave a patient looking a better version of their younger self for many years.

They don’t just look younger, they look more attractive. Additionally, there will be no tell tale signs of facelift surgery, the ear lobes and ear cartilages will remain unchanged, the volume shifts of ageing will have been addressed and even close family and friends will just think they look really well.
Take this patient, Helen, 5 months after composite deep plane face and neck lift, platysmaplasty and lateral brow lift. That seems like a lot of surgery but there are are no short cuts to a balanced facial rejuvenation. Patients want “less is more” but in the drive to do less – operated unbalanced results are being created.
The reality is more is less, if the face, neck, eyes and brow can be rejuvenated together, the ultimate result is far more pleasing, in proportion and less likely to be detected. I have marked the subtle changes the sum of which add up to make a facelift great – use it as a template for comparison.

How to assess before and after photos
So now you know what to specifically look for in a before and after facelift photo, let’s learn about the subtle stage tricks that can be used to improve the result.
All of the following are out there, marketing leaflets, review sites, galleries, press articles etc. Once you know about them you’ll see examples everywhere.

Smiling
It sounds obvious but it is extraordinary how many results are displayed with the patient at full smile in the after photo. A smile is a facelift in itself and elevates the mid face and jowls. Post facelift patients are generally smiling with their newfound confidence but I try to discourage smiling momentarily for the photo!

Positioning
An accurate comparison can only be made when the face is rotated to exactly the same position. Even a slight neck twist engages the neck muscles and can flatter a neck lift result.

Lighting
In a world lit from above, we don’t see jowls and wrinkles, we see shadows and creases. Both before and after should be with the same lighting. A flash minimises shadows and improves skin tone.

Make up
It’s difficult to ask patients to remove their make up for after pictures at post op review which is why I take my before photos at initial consultation for accurate comparison. A before without makeup and an after surgery with full make up is a common trick.

Neck chin angle
Even a 5 degree neck extension upwards can create a smoother jawline and reduce neck bands. Make sure before and after surgery profile views are taken a similar angles. Ideally after side profile photos with the neck flexed shows the integrity of lift perfectly.

Full ear visibility
It’s amazing how many before and afters don’t show the ears, but when you know why it becomes obvious. In the first few weeks after a facelift, the face is swollen and as swelling subsides, there is a stage where swelling acts like perfectly placed filler giving a very young and fresh appearance. At this stage post surgery, incisions and scars are highly visible which would indicate the final result is yet to be achieved and the before and after isn’t yet representative of the final outcome. Later ear covered photos might be hiding pixie ears and tension deformities.
How to choose a facelift surgeon
Facelift surgery recommendations by word of mouth
If you have seen facelift results first hand in a friend and like their transformation ask them who did it! I see facelift patients regularly who want a facial plastic surgeon in London, and over 60% came to me by word of mouth which brings me wonderful patients within a connected network of lovely people.
Do you like your prospective surgeon’s facelift surgery results?
Even great facelift surgeons on paper aren’t the best artists – facial rejuvenation is equally art and taste as it is science. Facelift surgeons create a signature look, ask to see lots and lots of standardised photos and take your time looking at them forensically. Look for longer term follow up and as the results from facelifting vary between patients for a myriad of reasons ask to see patients of a similar age, weight and ageing concern to yourself.
Does your face lift surgeon specialise in one area only?
The only way to become an expert is time, dedication and experience. When focus is split on all of body as well as face surgery, that expertise is diluted and it is more likely you will get a ‘standard’ facelift not one tailored to your specific needs.
Volume of Facelifts
is one thing, it is very easy to amass a large logbook of minilifts. Volume of quality facial surgery is key. How many full facelifts does your surgeon do a week and a year? Less than one a week or 50 a year and you have to question the focus and experience. More than four a week or 200 a year and you have to question the complexity (or not) of facelift, who is assisting, and when will your surgeon have time to see you for follow up.
Honesty, candour and humility
A good surgeon will gently decline to perform surgery if it’s not safe or he or she feels expectations of result aren’t aligned. You should feel positive about options after your consultation not worse that areas you hadn’t even noticed were highlighted as part of the consultation process. This is even more true for those seeking revision facelifting who have already had their confidence dented. All surgery carries risk, the greatest facelift surgeons get complications, it is inevitable – ask to see them and how they were managed. Ask to speak to previous patients at least a year out of surgery.
Gut feel
Probably the most important sign. Choosing to undergo facelift surgery is a big decision. A little like climbing a mountain. You want an experienced guide and team who will help you up safely and get you back down, helping you through the tough parts and enjoying the highs of the journey with you. Do you like your prospective surgeon and their team, it is important as they will be supporting you on a personal journey.

Cautions
As with all products and services, it is buyer beware. I have seen hundreds of revision facelift surgery patients from all over the world and there are common themes with their initial choice.
Heavy marketing
You’ve read about a facelift in a magazine, you’ve seen advert, a surgeon has paid for sponsored links on review sites. You have to ask yourself why word of mouth isn’t working?
Incentivisation
Time limited offers, free consultations, discounts and pressure selling are for end of line summer sales not surgery. Patients often consider surgery for years and should be given time to reflect and consider on an important decision.
Downplaying risks and recovery / Shows short term results
Both of these might suggest that what is being offered is minilifting where the underlying deeper soft tissue work is limited, longevity and result might be compromised.
Unable to show you hundreds of recent facelift outcomes
If you are considering facial surgery you want to see that your surgeon is technically evolved and is in their surgical prime. If you are being shown a selection of well thumbed printed photos it might be worth continuing your search!
Trademarked procedures
In my opinion we shouldn’t be able to trademark facelift surgery. A surgeon is constantly learning and evolving and the best surgeons learn and share ideas with each other to benefit all their patients. Trademarking a minilift, surgical procedure or technique gives patients the impression it is something unique – it isn’t, it’s a sales trick.
Competitive pricing
A facelift is not a something you should be shopping for in the bargain basement. The old adage buy cheap, buy twice is unfortunately true. It’s often a false economy, you could get lucky but is it worth the risk with cosmetic surgery?
Negatively commenting on others work
I have seen many a poor patient with a suboptimal facelift result seek my help for correction. They tell me that some surgeons almost delight in telling them how awful their result is and how it has to be fixed at great cost. This does nothing for their already low confidence. It is my rule never to comment negatively on a patient’s previous surgery, including medicolegal expert requests. Highlighting errors doesn’t fix the problem. What I can do is focus on how I can help them going forward.
The Psychology of Facelift Surgery
A candid analysis of drivers behind patient’s decisions to undergo facial rejuvenation surgery.
Discover more




